All pictures presented in this article have been downloaded from different sites in the internet through Google Images.The reader may find the source by searching the caption of each figure in Google Images.
Table of Contents
Some relevant statistics. 1
The Malady. 2
The basic background. 3
VESTIBULAR COMPENSATION and its importance in restoration of balance. 4
PHARMACOLOGICAL TREATMENT OF VERTIGO.. 6
COMMONLY USED DRUGS IN PATIENTS OF VERTIGO.. 6
Prochlorperazine. 8
Cinnarizine. 11
Dimenhydrinate. 15
Meclizine. 15
Betahistine. 15
Diazepam.. 16
OTHER DRUGS USED IN VERTIGO.. 16
NON PHARMACOLOGICAL TREATMENT OF VERTIGO.. 16
Physical therapy. 16
Counselling and Reassurance. 17
Recommendations. 17
Summary. 17
REFERENCES. 18
VESTIBULAR SEDATIVE DRUGS- reducing misuse why and how
Some relevant statistics
Disorders of the balance system affect a very large part of the population. Patients suffering from balance disorders present with head spinning, dizziness, imbalance, unsteadiness and associated symptoms. The overall incidence of balance disorders is 5-7% of the population and is as high as 35% in patients older than 40 years (1) and about 70% in patients above 65 yrs of age (2). International statistics report that 5-10% of the population presents to the doctor with vertigo / imbalance as a new case every year. The incidence of falls is 25% in subjects older than 65 years (1). Prevalence of balance disorders or dizziness is 15.8% of the population according to a study of Wiltink, J., R. Tschan, et al. (2009)(3).65% of individuals (older than 60 years of age) experience dizziness or loss of balance; often on a daily basis (4)(5). Indian statistics are not available but averages of published studies of prevalence of vertigo in different countries shows that 15% of the general population suffer from balance disorders.
Balance disorders are hence a very common disease that affects a very large part of the population. This makes the business potentiality of any drug that can be claimed to be helpful in balance disorders very attractive for commercial exploitation. In a one year span (October 2015 to Oct 2016) the sale of anti-vertigo drugs (comprising of just cinnarizine, flunarizine, betahsitine, and the cinnarizine + dimenhydrinate combination) in India was of about Rs 421.5 crores. There are other popular anti-vertigo drugs also like prochlorperazine and meclizine which if added would take the figure to above Rs.500 crores. In the month of October 2016 alone 757.7 lakh units of anti-vertigo medicines were sold.
The Malady
Balance disorders are a subjective disorder that causes physical, functional and psychological impairment and a social embarrassment that is not compatible with normal life. It imposes severe restrictions on the patient and also induces psychological disorders like anxiety, apprehension, insecurity and depression. Most balance disorder patients have a very poor quality of life with restricted mobility, persistent fear of losing balance or of falling down and a constant apprehension of impending vertigo. In addition to their physical impairment they are also mentally distressed. Hence patients suffering from balance disorders are a harried lot who would lurch at any opportunity for relief. This makes them easy target for any commercial endeavour. The enormity of the market for drugs than can be sold for the treatment of vertigo and / or balance disorders and the gullible patient’s hankering for trying out anything that promises relief from vertigo is therefore very luring to pharmaceutical companies. No wonder commercial interests overrule ethical and scientific therapeutic principles and influence the treatment of balance disorders. This is harmful to the interest of the patient. Pharmaceutical companies use all marketing means, if not gimmicks to promote the sale of such drugs paying scant attention to medical principles. This happens primarily because there are no restrictions on sale of these drugs (all these are available over the counter and are sold even without valid medical prescriptions) and because of the huge profit margins involved in the sale of these drugs. There is unethical, illogical and unscientific promotion of such medicines and even false propaganda leading to over-prescription and over-use. Vertigo and imbalance are such scary conditions for the patient that often patients are scared to stop the medicines and go on using them by purchasing the anti-vertigo medicines from medicine counters even after the patient is symptom free and is not having the vertigo or any imbalance. The medicines are erroneously used as a prophylaxis against vertigo/ imbalance which is medically wrong, scientifically irrational and logically untenable if not blatantly harmful. Even some naive medical practitioners prescribe these anti-vertigo medications prophylactically being fed with incorrect and biased information by the pharmaceutical companies. All the anti-vertigo medications are at best symptom relieving drugs and have no prophylactic or therapeutic role whatsoever. The loser in the deal is always the patient while all other stake holders profit from it.The outcome of this is dangerous as unnecessary long continued use of these drugs is detrimental to health of the patient. Use of these drugs beyond a specified period and beyond requirement actually damages the balance system and delays if not prevents the restoration of normal balance function some references of which are cited below. Most drugs used for management of balance disorders have serious side effects some of which is permanent. It is medically established that overuse of most of these drugs can completely jeopardise the natural process of restoration of balance (after the balance system has been damaged by disease). The process of restoration of balance after the balance organs have been damaged is a natural process called vestibular compensation and this is inhibited by most of the anti-vertigo medications. If the compensatory mechanism is jeopardised, the patient remains imbalanced and the normal balance function is not restored. Any imbalance is physically restrictive and mentally traumatic for the patient. Balance disorders induce psychological distress; balance disorders and psychological disorders are comorbid conditions and one perpetuates the other. Since balance disorders are so very common involving so many patients and since the impact on quality of life caused by balance disorders is so very severe, it is high time that an analysis and auditing of the management of balance disorders is undertaken. Nearly all drugs sold in the market that claim to cure balance disorders are OTC (over the counter) products and most do not come under any price restriction which is prevalent for many other drugs like antibiotics, anti diabetics , anti hypertensive and anti cancer drugs. Hence free sale of these are allowed and even a valid medical prescription is not mandated for the sale of these potentially dangerous and harmful drugs. The purpose of this document is to have an in-depth appraisal of the current scenario of management of balance disorders and offer solutions for corrective measures if not to make an attempt to stem the rot and thereby protect the hapless balance disorder patient from falling prey to the unscrupulous propaganda for anti-vertigo drugs . This is necessary since the currently prevalent practice of management of balance disorders esp pharmacotherapy appears unethical, injudicious, flawed and driven primarily by commercial considerations all of which are health-wise damaging and detrimental to the unfortunate balance disorder patients. This document not only highlights the ill effects of the anti vertigo drugs but advocates against overuse and unrestricted sale.
The basic background
The balance system is very complex and involves multiple organs and multiple systems of the human body; the vestibular labyrinth in the inner ear is one of them. Though the vestibular causes of imbalance are less than 50% (6) yet the drugs used to sedate the vestibular labyrinth are indiscriminately used in patients complaining of any of the symptoms like head spinning (vertigo), dizziness, light-headedness, unsteadiness, blackouts etc. without even ascertaining whether the vestibular labyrinth is really malfunctioning or whether sedating the vestibular labyrinths is actually necessary or not. The drugs used to sedate the vestibular labyrinth are called vestibular sedatives or anti-vertigo drugs.These drugs do much more harm than benefit and are capable of only providing temporary relief from the symptom of acute vertigo or head spinning. Serious adverse effects of these drugs can range from Parkinsonism (7) to even life threatening Neuroleptic Malignant syndrome(8) .The biggest drawback is that these drugs jeopardise the natural process by which the normal balance function is restored after it has been damaged by disease. The vestibular labyrinths are made of special sensory epithelium that detect movement very much like the retina in the eyes that detects light and is responsible for our vision and the cochlea in the ear that detects sound and is responsible for our hearing. All special sensory epithelium cells are made of cells that are non-mitotic and once damaged are damaged for life i.e., they do not regenerate. The anti-vertigo drugs or for that matter any medicine cannot regenerate the cells of the vestibular labyrinth if dead. The purpose of the anti vertigo drugs is just to provide symptomatic relief from any rotating / spinning sensation if there is any and that too only temporarily even though they are unscrupulously touted by the pharmaceutical companies as the panacea for all diseases that manifest as vertigo or imbalance. The anti-vertigo drugs are vestibular suppressants and suppress the sensitivity and functioning of the vestibular labyrinth. If there is no spinning sensation i.e., if the feeling is that of instability / dizziness/ blackouts / sinking anti-vertigo drugs have no role whatsoever. The head spinning i,e. the spinning / rotatory sensation felt by the patient which is called true vertigo or even the related sensations like instability dizziness, sinking sensation are just the manifestation of some underlying disease and are not a disease in itself. The doctor’s job is to ascertain / diagnose the cause of the vertigo and the other symptoms and treat the underlying disease instead of camouflaging / suppressing the symptom of vertigo.
Most of the vestibular disorders that cause vertigo /imbalance have specific therapies which do not require treatment with the vestibular sedative (or anti-vertigo) drugs. The mainstay of treatment remains vestibular rehabilitation and specific treatment directed to the disease that is causing the vertigo /imbalance. The vestibular compensation mechanism which helps a balance disorder person to recover and get back the normal balance function is also hampered by these drugs and long term use of such drugs leads to a permanent instability which cannot be cured by any means. Some of these drugs which are available as OTC products in our country with all chemists are actually not approved by Food and Drug Adminstration (FDA) of USA. Other developed countries also have strict regulations for these drugs.
These drugs do have a limited role in relieving the symptom of head spinning but only in the acute stages of the disease and should not be used for more than 3-5 days (9)(10)(11)(12). Use of these merely symptom relieving drugs for vertigo camouflages the underlying disease which remains undiagnosed, induces a false sense of complacency both in the patient and on the doctor and what is worst is that it also jeopardises the natural process of restoration of balance. This policy paper is presented to highlight this particular aspect and to recommend enlisting these drugs in schedule H so that they cannot be sold without valid medical prescriptions and also to bring all these drugs under price bar so that the profitability is reduced. The later will ensure that the over hyped advertisement and mindless promotion among doctors for the anti-vertigo drugs by the pharmaceutical companies which is sending wrong signals to all stake-holders is reduced.
VESTIBULAR COMPENSATION and its importance in restoration of balance
Vestibular compensation is a unique corrective mechanism ingrained in the human biological system wherein there is reorganization of internal connections of the brain which helps in maintaining the balance in spite of a lesion in the vestibular labyrinth. But for this to occur, brain needs inputs from the vestibular labyrinths in the form of vertigo.
For vestibular compensation to occur sensory input in the form of vertigo is of utmost importance. This helps brain to understand that there is difference in sensitivity of both labyrinths (termed as ‘sensory conflict’ in medical parlance) and that one of them is hypo-functioning or working at suboptimal levels; hence the internal connections are reorganised and recalibrated accordingly. More the sensory conflict, more is the vertigo and better is the compensation (9)(10).
Any drug which reduces the sensory conflict by reducing the feeling of vertigo hampers the process of compensation. There is no drug with adequate and convincing evidence to claim that it helps i.e., enhances / expedites the process of compensation (9) (Figure 1). On the other hand it is known that any drug that depresses the central nervous system (CNS) jeopardises vestibular compensation. Most drugs that are used for supressing vertigo actually depresses the CNS except for betahistine which is not a CNS depressant. But as it reduces the symptom of vertigo it definitely reduces the sensory conflict and hence also inhibits vestibular compensation though may be at a lesser level than the other anti-vertigo drugs all of which depresses the CNS. The compensatory mechanism in the brain is most active in the first few days after a vestibular assault, hence one has to be very discerning in supressing vertigo with the anti vertigo drugs when there is an acute damage to the vestibular labyrinth.
PHARMACOLOGICAL TREATMENT OF VERTIGO
Objectives for medical treatments of vertigo are as follows (9):
- Reduction/ cessation of the symptom of vertigo;
- The enhancement -or at least non-reduction – of the processes of ‘vestibular compensation’ to allow the brain to formulate a new sensory equilibrium in spite of the vestibular lesion; and
- The reduction of neurovegetative and psychoaffective signs (nausea, vomiting, anxiety) that often accompany vertigo.
COMMONLY USED DRUGS IN PATIENTS OF VERTIGO
Following are the commonly used drugs in the treatment of vertigo.
– Prochlorperazine – Cinnarizine
– Dimennhydrinate – Betahistine
– Meclizine – Diazepam
All of these drugs are discussed in details in the following pages, but there are few common points to all of these drugs. Prochlorperazine, cinnarizine, dimenhydrinate and meclizine are antihistaminic anti cholinergic drugs and hence share the same effects and adverse effects with minor variations. Betahistine is a histamine analogue and acts differently but no doubt has a anti vertigo effect.
- All these drugs decrease the sensitivity of vestibular labyrinth and hence affect the vestibular compensation.
- All these drugs should be used only and only as a symptom relieving measure for 3-5 days (9)(10)(11)(12) at the most, not beyond that.
- None of these drugs have any curative role in any disease of the vestibular system whatsoever. The only exception is betahistine which is believed to have some curative effect in confirmed Meniere’s disease. But Meniere’s disease is not a very common cause of vertigo in our country and it has very specific characters by which it can be identified.
- The anti-vertigo effect of all these drugs are obtained from one or more of the following mechanisms viz. blocking receptors in the higher vestibular pathways and thereby inhibiting neural transmission in the brain, reducing the firing rate in the vestibular labyrinths, depression of the CNS. All these process inhibit vestibular compensation which males these drugs detrimental to restoration of normal balance function.
Michel Lacour has mentioned in 2006 scientific paper (figure 2), that following a sudden unilateral vestibular loss, patients exhibit incapacitating symptoms, such as nausea, vomiting and vertigo. These symptoms can be stopped or limited using vestibular suppressive drugs. However, as the literature suggests that drugs with sedative effects slow down the recovery process, it is therefore recommended that these agents are prescribed for a limited period of time, and that the use is restricted to the first 3 or 4 days after an acute vestibular loss.(13)(9)
Baloh R was mentioned in Vestibular Rehabilitation book that drugs exerting sedative effect on Vestibular system should be used only first 24hrs (11)(12)(Figure 3).
Mukherjee et al mentioned in in an article on vertigo and dizziness (Figure 4) that- Vestibular suppressants should be prescribed over a limited period of time following an acute vestibular lesion. Chronic use is not advocated as it probably retards the process of central vestibular compensation. A process of rehabilitation should be started after the acute phase and this includes vestibular rehabilitative exercise. Vestibular suppressants and other central depressant medicine should be discontinued as both can interfere with the adaptive plasticity considered the basis for successful rehabilitation. (14)
These drugs are commonly used in patients of vertigo. They are often misused and are also available over the counter (OTC). We are discussing over here the mechanism of action and harmful effects of these drugs on individual basis.
Prochlorperazine
Belongs to the phenothiazine group of antipsychotics.. Antipsychotic drugs are tranquilisers that are used to treat serious mental disorders like schizophrenia, bipolar disorders, depression, mania, hallucinations, delusions and similar mental states. Though it is used to treat dizziness it itself may induce dizziness and vomiting in addition to, drowsiness restlessness., constipation, and dry mouth in patients when prescribed as these are the common side effects of all antipsychotic drugs. Though prochlorperazine offers very good symptomatic relief in acute vertigo yet, it is an antipsychotic drug meant for serious mental disorders with many untoward effects and so should be used with utmost caution.
Prochlorperazine has following pharmacological effects –
- Antihistaminic (H1)–action by which it antagonizes actions of histamine or the subclass of histamine receptors (H1 or H2) found on tissue.
- Anticholinergic effect which acts by iinhibiting or blocking the physiological action of acetylcholine which is a neurotransmitter at nerve endings of many nerves in the brain and other parts of the CNS. Neurotransmitters conduct the passage of neural impulses from one nerve to another. Anti-cholinergic effect blocks neural transmission in the cholinergic pathways of the brain. Unfortunately many activities of the brain including the process of vestibular compensation occur through the cholinergic pathways. So an anticholinergic drug inhibits many neural activities in the brain and hence acts as a CNS depressant and worse of all it also inhibits vestibular compensation.
- Antidopaminergic(D2)– effect acts by blocking the neurotransmitter dopamine thereby preventing or countering dopamine effects. Dopamine is a neurotransmitter in the central nervous system, peripheral nervous system and in the blood vessels. It is a very important chemical in the basal ganglia causing muscle rigidity tremor, depression etc. Reduced levels of dopamine in the basal ganglia causes extra-pyramidal disorders like Parkinsonism. Antidopaminergic effects are discussed in more details in the section under cinnarizine.
Following are the possible adverse effects of prochlorperazine
- Extrapyramidal effects like acute dystonic reactions (Figure 9), oculogyric crises (Figure 5), pseudo Parkinsonism and akathisia (Figure 8) are the major drawbacks – more common in children and adolescents.
- Opisthotonus (Figure 7), Spasticity (Figure 13), Blepharospasm(Figure 6), Macroglossia(Figure 11), Torticollis(Figure 10), Laryngospasm(Figure 12)
- Can also cause a life threatening condition called neuroleptic malignant syndrome(Figure 14)
- Hypotension, esp orthostatic hypotension can occur. i.e., patients taking prochlorperazine may have an abrupt fall of blood pressure on suddenly standing up from sitting / lying down position and may fall or sometimes even lose consciousness for a moment
- Anti-cholinergic effects (discussed below under cinnarizine) are often distressing for the patient and increases the morbidity of the patient
- Since it causes CNS depression it jeopardizes the much needed vestibular compensation which is essential to restore balance


Figure 5 Oculogyric Crisis








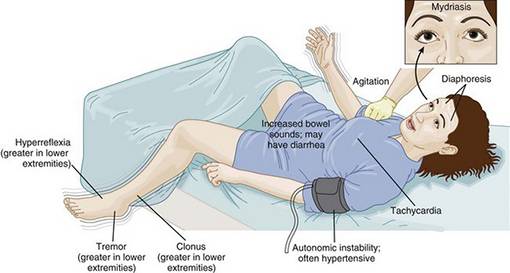
Figure 14 Neuroleptic Malignant Syndrome(15)
Cinnarizine
Has following mechanisms of action
- Anticholinergic – blocks cholinergic transmission in the brain which includes the neural pathways for vestibular compensation
- Antidopaminergic – blocks D2 receptors and block the release of dopamine which in turn induces mental depression and other psychological and physiological abnormalities
- Ca – channel blocker – prevents entry of Ca-ions in the labyrinthine cells and in the smooth muscles of blood vessels
- Anti-serotonergic properties by which it antagonises serotonin. Serotonin is a neurotransmitter which regulates motility in the gastrointestinal system and provides sense of wellbeing. The anti-serotonrergic effect hence indices constipation flatulence and makes the patient depressed
It provides a good symptomatic relief to the patient but its side effects outweigh the benefits and hence this drug is best avoided more so because we have other alternatives.
Following is the list of adverse effects of cinnarizine
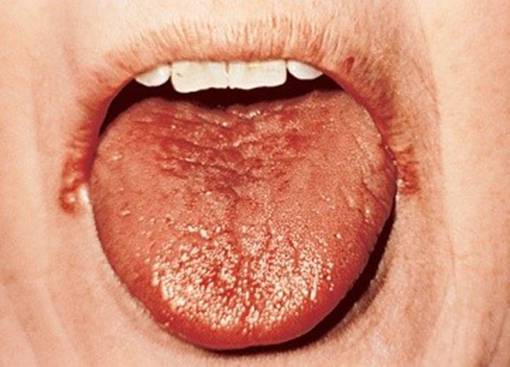
- Due to anticholinergic properties(16) –
- Xerostomia(Figure 15)
- Dry sore throat
- Warm,blotchy,red skin due to decreased epidermal thermal dissipation
- Increased body temperature
- Mydriasis,photophobia(Figure 17)
- Cycloplegia-loss of accomodation
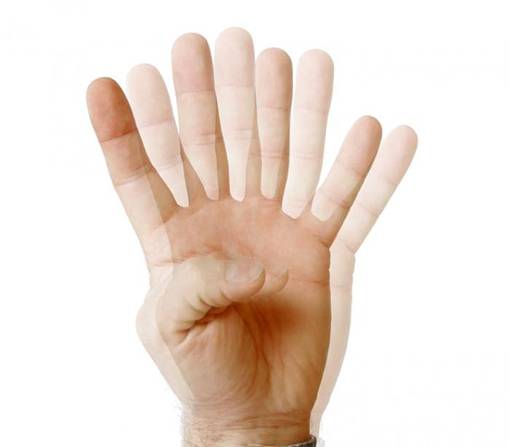
- Diplopia (Figure 16)
- Increased intraocular pressure
- Loss of coordination
- Tremors (Figure 18)
- Tendency to be easily startled
- Tachycardia
- Urinary retention
- Diminished bowel movement-sometimes paralytic ileus i.e., intestinal obstruction
The anticholinergic effect induces CNS depression and drowsiness by virtue of which the vestibular compensatory mechanism is inhibited


- Due to anti-dopaminergic properties (due to prevention of MgATP dependent production of electrochemical gradient-lowered level of dopamine in basal ganglia neurons) (17)
- Depression (Figure 19)
- Tremor (Figure 18)
- Muscle rigidity
- Akathisia(Figure 8)
- Tardive dyskinesia (Figure 20)
- Drug induced Parkinsonism-due to its affinity for the D2 receptors in the stratum of brain(Figure 21)(7)(18)
- Due to Calcium channel blocking
- affect depolarization in SA and AV node and also affect AV conduction by which a negative inotropic effect is produced in the cardiac cells
- Pedal edema occurs as smooth muscles in vascular wall are prevented to contract
- Throbbing headaches occur commonly
- Labyrinthine sedative effect by which it provides reasonably good symptomatic relief
- Anti-vasoconstrictive effect which helps in reduces slugging phenomenon of blood in narrow blood vessels and also stabilises vascular endothelium
Dimenhydrinate
- Conventional antihistaminic with high anti-cholinergic activity. Has very good antiemetic effect and hence provides relief not only from acute vertigo but also from the accompanying vegetative symptoms
- Common Adverse effects of Dimenhydrinate
- Highly sedative- hence impairs psychomotor skill. Concomitant use of alcohol or other CNS depressant should thus be discouraged.(Figure 22)
- Best avoided in breastfeeding mothers
- Better avoided in patients having enlarged prostate, glaucoma, emphysema, chronic bronchitis. – applies to other anticholinergics too
- At very high doses it can affect colour discrimination, night vision, visual reaction time, and stereopsis.
 Figure 22 Drowsiness
Figure 22 Drowsiness
Meclizine
Best used for symptomatic relief and hence use like for all other anti vertigo drugs should be limited to a maximum of 3-5 days or as soon as the symptom is relieved whichever is earlier. Competitively antagonizes the actions of histamine at H1 receptors. Its main advantage is that the anticholinergic effects are lesser compared to other conventional antihistaminic antivertigo drugs like prochlorpearzine, cinnarizine and dimenhydrinate. It is approved as OTC product by FDA hence safety profile is comparatively much better than the other anti vertigo drugs
Adverse effects of meclizine are due to both anticholinergic and antihistaminic properties which have been elaborated earlier but the effects are much milder in nature.
Betahistine
It is a anti-vertigo drug without any CNS depressive effects. It provides symptomatic relief in vertigo by its action on some histaminergic receptors in the higher vestibular pathways. It has been shown to be effective in the treatment of Meniere’s disease which is one of the not so common causes of vertigo.
- Structural analogue of histamine
- Agonistic action on H1 receptors
- Antagonistic action on H3 receptors
Adverse Effects of Betahistine
- Different allergic and skin related side effects and hypersensitivity reactions like tingling, numbness, burning sensation, respiratory distress can occur due to increased histamine level
- To be used with caution in asthmatics and peptic ulcer pts as it is a mild H2 agonist and can enhance gastric secretion
- Systemic administration causes peripheral vasodilatation and a fall in systemic blood pressure-so use of very high dose should be avoided.
Diazepam
It is a very good anxiolytic and has a CNS depressive effect and by this provides symptomatic relief in acute vertigo. As it is a CNF depressant just one or two doses to control symptoms in very acute stage is the most that is allowable. It has tranquilising & anxiolytic effects. Since it decreases resting activity of vestibular nuclei ; hence provides symptomatic relief. It acts upon the reticular formation and limbic systems in the brain hence reduces concomitant anxietyBut as it is a CNS depressant it should best be totally avoided.
OTHER DRUGS USED IN VERTIGO
Apart from the above drugs which are basically symptom relieving medicines, pharmacological treatment of vertigo should be directed towards treating the underlying disease causing the vertigo after identifying it. Treatment includes drugs for migraine prophylaxis, diuretics, anti epileptics, steroids, anti-virals, antibiotics, SSRIs, benzodiazepines, nootropic agents, anti-oxidants etc.
NON PHARMACOLOGICAL TREATMENT OF VERTIGO
Physical therapy
Various types of physical therapy especially excercises like Cawthorne Cooksey Excercises; Yogic Asanas; Tai Chi excercises are recommended for vestibular rehabilitation and promoting of vestibular compensation. Depending on which part of vestibular labyrinth is involved specific exercises are available and many more are being developed helping the person to lead a normal life. For disorders like positional vertigo, the different liberatory manoeuvres work wonders. The commonest cause of vertigo in any clinic that can diagnose the cause of the vertigo is a disorder called Benign Paroxysmal Positional Vertigo (BPPV) for which there is no medical cure and can be corrected by different physical therapies called liberatory manoeuvres then and there in the clinic itself. In spite of this, patients of BPPV are prescribed medicines for prolonged periods which they continue even after the BPPV gets corrected by itself. BPPV like some other causes of vertigo is a self limiting condition that is corrected in a few days without any treatment
Counselling and Reassurance
This is the most important aspect of treatment as the patient needs to be reassured about his condition and also to overcome his apprehension and anxiety. Very often some psychological impairment co-exists which requires counselling.
Recommendations
The relevant authorities like drug controllers and health care regulatory bodies should take steps to:-
- Bring all anti-vertigo medicines under a fixed price bar so that the profitability is reduced.
- Make wrong propaganda and irrational promotion of medicines by pharmaceutical companies a punishable offence
- Introduce auditing of prescriptions so that medicines and the dosage prescribed by doctors is medically justifiable at least for the anti-vertigo drugs. A suitable legislation will be a effective deterrent for irrational prescriptions.
- Bring all anti-vertigo drugs under schedule H, so that these drugs cannot be sold without a valid medical prescription.
Summary
Vertigo and imbalance are very common disorders which not only cause a severe physical morbidity and also have a psychological impact both of which together bring about a poor quality of life in the patient. However both vertigo and imbalance are not a disease in themselves. Like fever and pain, vertigo / imbalance is just a symptom or manifestation of an underlying causative disorder. This underlying cause needs to be diagnosed and treated. Unfortunately, the current trend in medical practice is to treat vertigo and imbalance by symptom relieving anti-vertigo drugs which camouflage the underlying disorder without in any way curing the causative pathology. This happens primarily because of the hype in promotion of the anti-vertigo drugs which are touted by different pharmacological companies selling them as the panacea for vertigo and imbalance irrespective of the cause. The pharmaceutical companies promote the long continued use of the anti vertigo drugs using different marketing gimmicks and use different tricks of disinformation and misinformation to convince doctors on the curative effects of the anti vertigo drugs. Their professional marketing strategies easily dupe naive doctors into towing their line. This results in over-prescription and irrational use of the anti-vertigo drugs. The price for this in terms of health and money is paid by the hapless patient. All the anti-vertigo drugs have very serious side effects and even prevent the proper development of a natural corrective process called ‘vestibular compensation’ ingrained in our systems which actually restores balance after the balance organs have been damaged by disease. If the vestibular compensation does not take place as desired, the patient remains imbalanced which has a serious impact on the physical and mental wellbeing of the patient. Persistent vertigo and imbalance causes a sense of insecurity, fear and other psychological disorders like mental depression and anxiety. These psychological conditions further augment the imbalance and starts a vicious cycle where one perpetuates the other. The current consensus among neurotologists (medical specialists who specialise in the treatment of vertigo/ imbalance) is that anti-vertigo drugs should never be used for more than 3-5 days. In fact some authorities recommend that they should not be used for more than 24 hours. But the scenario in medical practice is completely different and doctors are found to prescribe these drugs for weeks and months together and what is worse is that patients then go on taking these drugs by purchasing them over the counter for years at a stretch. The impact of this on the balance system is very bad and most such patients develop a permanent instability and consequently a very poor quality of life more so because of the induced psychological impact caused by the balance disorder. What was once a correctable / controllable medical disorder now becomes unmanageable and the patient becomes a wreck more mentally than physically because of the persistent imbalance induced by the irrational and unscientific therapy which is totally against medical consensus. The underlying disease remains undiagnosed and progresses unabated. This is a real menace and drastic steps, if not ‘surgical strikes’ need to be taken immediately to stop this illogical and harmful practice of prolonged use of anti-vertigo drugs. Some recommendations are presented in the document.
REFERENCES
- Samy, Hesham M, Hamid, Mohamed A and Friedman, Marc. Dizziness, Vertigo, and Imbalance. Medscape. [Online] 29 11 2016. http://emedicine.medscape.com/article/2149881-overview#showall.
- Balance disorders in the elderly: epidemiology and functional impact. Lin, H W and Bhattacharyya, N. 8, August 2012, Laryngoscope, Vol. 122, pp. 1858-1861.
- Dizziness: anxiety, health care utilization and health behavior–results from a representative German community survey. Wiltink, J. and Tschan, R. 5, 2009, J Psychosom Res, Vol. 66, pp. 417-424.
- What Causes Dizziness / Vertigo. http://nationaldizzyandbalancecenter.com/. [Online] http://nationaldizzyandbalancecenter.com/resources/what-causes-dizziness-vertigo/.
- Equilibrium and balance in the elderly. Hobeika, C P. 8, August 1999, Ear Nose Throat J, Vol. 78, pp. 558-566.
- Hain, Timothy. Epidemiology of Dizziness. http://dizziness-and-balance.com/. [Online] [Cited: 11 Sep 2014.] http://dizziness-and-balance.com/disorders/dizzy_epi.html.
- Drug induced parkinsonism A review. Hirose, Genjiro. Suppl 3, 2006, J Neurol, Vol. 253, pp. III/22 – III/24.
- Theodore, Benzer and Mancini, Mary C. Neuroleptic Malignant Syndrome. Medscape, Drugs & Diseases. [Online] http://emedicine.medscape.com/article/816018-overview.
- Antivertigo Medications and Drug-Induced Vertigo A Pharmacological Review. Rascol, Olivier, et al. 5, 1995, Drugs, Vol. 50, pp. 777-791.
- Hain, Timothy C. Drug Treatment of Vertigo. Dizziness and Balance. [Online] [Cited: 30 August 2015.] http://www.dizziness-and-balance.com/treatment/drug/drugrx.html.
- Herdman, Susan J. and Clendaniel, Richard. Vestibular Rehabilitation (Contemporary Perspectives in Rehabilitation) 4th Edition. 4th Edition. Philadelphia : F.A. Davis Company Philadelphia, 2014. p. 253 Chapter 14. ISBN-13: 978-0803639706; ISBN-10: 0803639708.
- Baloh, R W and Kerber, K A. Clinical Neurophysiology of the Vestibular System. Fourth Edition. New York : Oxford University Press, 2011.
- Restoration of vestibular function: basic aspects and practical advances for rehabilitation. Lacour, Michel. 9, 2006, Current Medical Research and Opinion, Vol. 22, pp. 1651-1659.
- Vertigo and Dizziness — A Clinical Approach. Mukherjee, A, Chatterjee, S K and Chakravarty, A. November 2003, JAPI, Vol. 51, pp. 1095-1101.
- Nursing crib. http://nursingcrib.com/nursing-notes-reviewer/psychiatric-mental-health-nursing/neuroleptic-malignant-syndrome/. [Online] http://nursingcrib.com/nursing-notes-reviewer/psychiatric-mental-health-nursing/neuroleptic-malignant-syndrome/.
- Anticholinergic side-effects of drugs in the elderly. Mintzer, Jacobo and Burns, Alistair. September 2000, Journal of the Royal Society of Medicine, Vol. Volume 93.
- D2 Receptor Blockade by Flunarizine and Cinnarizine Explains Extrapyramidal Side Effects. A SPECT Study. Brucke, T., et al. 1995, Journal of Cerebral Blood Flow and Metabolism, Vol. 15, pp. 513-518.
- Drug-induced parkinsonism: Cinnarizine and flunarizine are potent uncouplers of the vacuolar H+-ATPase in catecholamine storage vesicles.Terland, Ole and Flatmark, Torgeir. 1999, Neuropharmacology, Vol. 38, pp. 879-882.
- Dizziness presentations in U.S. emergency departments, 1995-2004. KA, Kerber, et al. 8, August 2008, Acad Emerg Med., Vol. 15, pp. 744-750.
- Rising annual costs of dizziness presentations to U.S. emergency departments. AS, Saber Tehrani, et al. 7, July 2013, Acad Emerg Med., Vol. 20, pp. 689-696.
- Dizziness: State of the science. Sloan, P D. 9 pt 2, 1 May 2001, Ann Intern Med, Vol. 134, pp. 823-832.
- Department of Otolaryngology – Head & Neck Surgery, Vestibular & Balance Center. University of Virginia Health System. [Online] http://www.healthsystem.Virginia.edu/internet/otolaryngology/patient_vbc.cfm.